PART I – DEFINITIONS, APPLICATIONS, COMPOUNDING AND INTERACTIONS
The rise of the medical and pharmaceutical industries, has led to the development of products designed to reduce human suffering and prolong life. Over several decades, materials such as metals, ceramics and polymers have been used to produce devices created to improve the health and quality of life. The biomaterials used are typically polymers, natural rubbers, polyurethanes, and silicone rubbers. Although the use of natural rubber can cause allergic reactions in some individuals, in general polymers can be “designed” according to the specific biomedical application and with special characteristics [1].
Silicone rubber (and Liquid Silicone Rubber) have good mechanical properties, are low cost, and are nontoxic and non-irritant materials. Because of theses desirable characteristics, it is considered a biomaterial [2]. By definition, a biomaterial is “a material, synthetic or natural, used in a biomedical device designed to replace part of a living system or to function in intimate contact with the living body for an intended method of application and for an intended period” [3]. First, it is necessary to distinguish the differences between biocompatibility and biostability. Biocompatibility is “the ability of a material to be in contact with a living system without producing an adverse effect” [4]. Biostability is “the ability of a material to adequately resist the degrading effects of the host” [5]. When a material loses biostability, it is no longer biocompatible. Biocompatibility depends on two factors: bulk properties and surface properties. Bulk properties are related to the function (mechanical) of the device − the mechanical interaction between the device and the surrounding tissues (weight, shape, flexibility), in other words, it must be a match to the set of properties of both [6]. The surface properties are related to the chemical and biological interaction between the material and the tissues [7]. Any device implanted or in contact with the body is designed to have a minimal impact on it. The response of the body will depend on the chemical composition of the surface [6]. Figure 1 shows the division of the biocompatibility of the material by properties, and Table 1 shows the key properties of silicone rubber to be used in biomedical applications [8].
Figure 1 Biocompatibility [5]
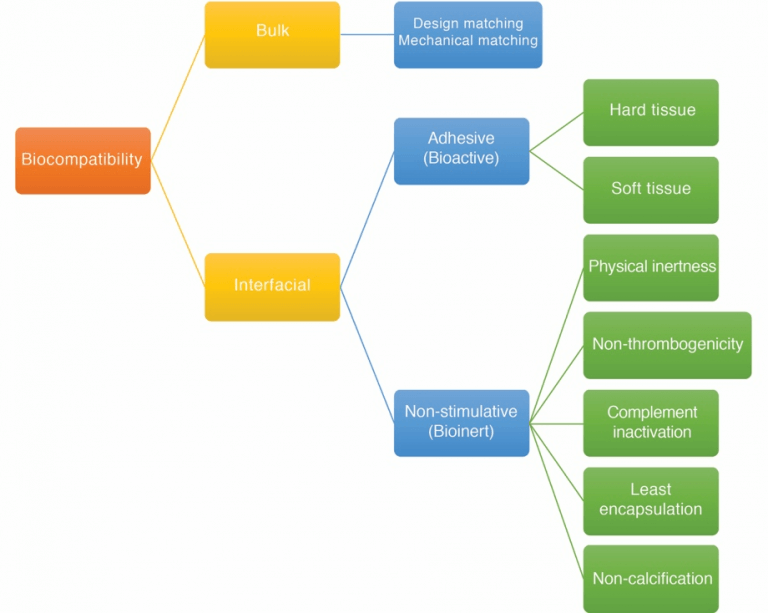
Table 1 Key properties of silicone rubber used in biomedical applications [8]
| Biological | Physicochemical |
| Non-toxic/inertness | Thermal stability |
| Moderate biocompatibility | Resistance to UV, oxygen, ozone and sunlight |
| Protein absorption | Resistance to aging and biodegradation |
| Hemocompatibility | Can be sterilized and has low curing temperature |
| Microbial adhesion | Excellent dielectric behavior
Low density and high molecular weight Chemical stability, resistance to hydrocarbons, oils and solvents Flexibility/elastic, easy to mold and shape High gas permeability Good optical transparency Hydrophobic character |
STERILIZATION
The Liquid Silicone Rubber (LSR) material used in biomedical applications must be able to be sterilized. Normally, the sterilization process is done between 110°C and 190°C in a dry or steam atmosphere and sometimes with pressure.
Gases are also sometimes used for sterilizing. Ethylene oxide gas (EOG) is one method of sterilization. The amount of EOG residue on the surface of silicone rubber devices is small because CO2 displaces any EOG absorbed. ClO2 gas is also used, however it creates changes in the LSR’s crystallinity and plasticization level after the sterilization.
Hydrogen peroxide is another method used for sterilization, however it is not recommended for used with silicone rubbers because it is largely absorbed during the process, increasing its cytotoxicity (the level of toxicity into the cells).
A method of sterilization that is becoming popular is Gamma irradiation. It has gained popularity because it does not involve toxic materials, but the irradiation causes scission in the silicone rubber molecules, changing the mechanical properties and even the crosslinking [9].
BIOMEDICAL APPLICATIONS
The advantages of using medical grade Liquid Silicone Rubber in biomedical applications are it is easy to process and its stability in contact with tissues in living organisms. LSR’s inherent hydrophobicity (material which repels water), however has caused some problems in the some devices over a long period of time (until now).
The Health Industry Manufacturers Association has classified medical devices into four categories as shown in Table 2. Liquid Silicone Rubber is used in all four categories, with more prevalence in I and II [9].
Table 1 Grouping of Medical Devices [9].
| Type | Environment | Duration | Application |
| I | Internal devices | Less than 30 days
More than 30 days |
Intravenous catheters
Drainage tubes Hip implants Pacemakers Artificial heart valves |
| II | External devices | Less than 30 days
More than 30 days |
Devices that contact the skin such as gloves, tapes, dressings and orthopedic casts
Devices that contact the mucous membranes such as urinary catheters and intravaginal devices |
| III | Indirect devices(No contact with the body) | Hypodermic syringes
Transfusion assemblies Dialysis components |
|
| IV | Non-patient contact devices(No touch the body) | Dressing trays
Packaging materials |
For many years, silicone rubber has been used in clinical implants because of its inherent bio-inert nature [10]. The most high profile application is the mammary prostheses, however this is just one of many applications. Figure 2 illustrates the prevalence and location of silicone rubber devices/implants in the human body, and in Table 2 the various implant applications.
Figure 2 Medical devices made from silicone rubbers in the human body [9].
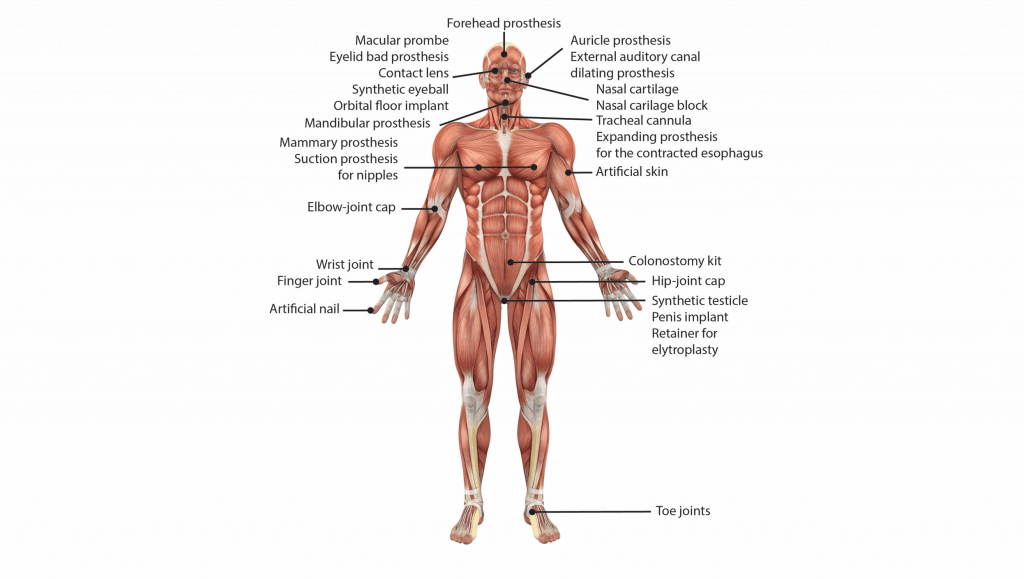
Table 2 Implant applications of Liquid Silicone Rubber [9].
| Treatment | Application |
| Plastic and reconstructive surgery | Reconstruction of nose, chin, ear armature, etc.
Breast reconstruction |
| Ophthalmology | Correction of detached retina
Prosthetic eye Repairing fracture of the floor of the orbit |
| Orthopedic surgery | Reconstruction of fingers, thumbs, wrists, elbows, feet, tendons, temporomandibular joint, etc.
Maxillofacial prosthesis Penile prosthesis |
| Cardiovascular surgery | Ball in the ball-and-cage heart valve
Coatings on pacemakers and lead-wires Construction in artificial hearts and hear assist devices |
The first reported use of silicone rubber in the human body were in the 1940s and 1950s. The first biomedical applications using silicone rubber were for the replacement of elastic elements of the human body, taking advantage of the inherent dynamic deformation of the material [10]; and used as a hydrocephalus shunt drain fluid from the brain [9]. In the 1960s, silicone rubber was utilized as an elastic, odorless and biocompatible material for reconstruction of facial structures used in facial and oral cancer surgery patients; and replaced polyethylene for use as artificial heart valves (the aortic, mitral and tricuspid cardiac valve). Silicone rubbers have also been used in dental liners, impression materials, and bands [11]. The first successful implant made of silicone was in breast implants.
Silicone rubber is commonly used in implanted cuff electrodes for both recording and stimulating peripheral nerves [12], and these electrodes are for long-term implantation. It can also be found in cardiac pacemakers, cochlear implants, artificial skins, contact lenses, oxygenators, catheters, and drug delivery systems [2]. In artificial skins, a bilayer of cross-linked collagen and chondroitin 6-sulfate is placed over a top layer of silicone. It serves well for traumatic and regenerative stages of skin replacement and prevents fluid loss and the proliferation of bacteria [9]. Using its high oxygen and CO2 permeability, it is used in the blood oxygenator membrane, as well as long wear contact lenses.
An interesting application is its use as drug delivery medium. A drug core is surrounded by a silicone membrane through which the drug will be released. In 1964, it was used for the first time to release digoxin, a low molecular weight drug [1], and currently is used in devices used to release progesterone, testosterone, spermicides, anti-inflammatories, antimicrobials, and anticancer drugs.
Silicone rubber is also being used in tissue engineering, and used in scaffolds, which are structures or framework that hold cells or tissues. The material must allow the adhesion, distribution, and proliferation of the cells, which reflects the difference with other applications (see discussion to follow: Interaction between Silicone Rubber and Cells, Tissues). Taking advantage of the hydrophobic nature of silicone rubber, certain compounds can be encapsulated in the scaffold for use as a slow release agent or platform for drug delivery [13].
Silicone rubber combined with NiTi (Nitinol) is being used in stents which require small variation of length during radial or bulge solicitations. This application takes advantage of the super-elasticity and shape memory behavior of NiTi and silicone rubber’s hyper-elasticity with permanent set [14].
COMPOUNDING RTVS AND LSRS FOR BIOMEDICAL APPLICATIONS
In biomedical applications, both Room Temperature Vulcanization (RTV) silicone rubber and Liquid Silicone Rubber (LSR) are employed. The conditions that must be met are: (i) after the vulcanization reaction there can be no presence of by-products, because after a certain time, they could migrate and come into contact with body fluids causing infections or encapsulation. To address this, the addition-type silicone rubbers are the best option due to their lack of by-products after the reaction. (ii) The components of the silicone rubber must not include any carcinogenic, thrombogenic, or toxic, allergic, or inflammatory materials.
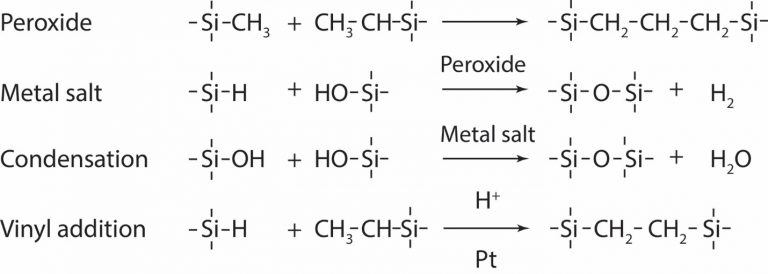
The RTV silicone rubbers used are two-part materials based on polydimethylsiloxanes (PDMS) vulcanized with platinum, organoplatinum, low molecular tetra(alkyloxysilane), stannous octoate, or through irradiation curing where the scission of C-H and C-Si bonds generates the crosslinking [1]. For Liquid Silicone Rubbers, two-part LSRs are also used with peroxides, metal salt, condensation, and vinyl addition as curing systems (Figure 3) [9].
Figure 3 Liquid Silicone Rubber curing systems [8]
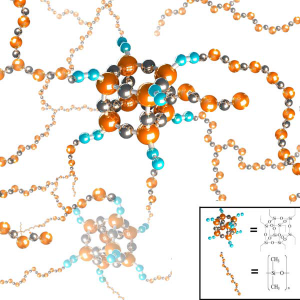
Usually, the fillers used in the compounding are inorganic (fumed silica, carbon black, TiO2), and for the biomedical applications, they are not adequate because fillers are not bound to the silicone backbones, and some of them are hazardous to the body. They can be replaced by Polyhedral Oligosilsesquioxane (POSS) catalysts. POSS catalysts are incorporated into the silicone during the vulcanization reaction, becoming chemically bound (Figure 4) [15].
Figure 4 Modified LSR and individual components for biomedical applications [15]
A 3D printing process has been developed for the direct fabrication of customized Polydimethylsiloxane (PDMS) implants using a compound similar to the conventional medical grade. Because of its inherent low viscosity, complex geometries can be made with a high-speed infrared curing system [16].
INTERACTION BETWEEN SILICONE RUBBER AND CELLS, TISSUES
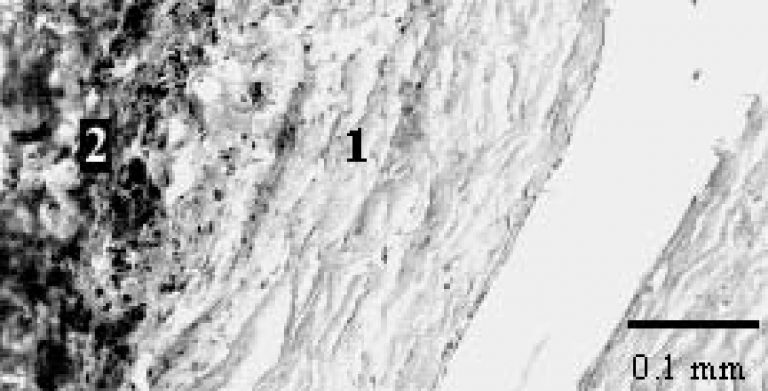
The cell-silicone rubber interaction is dependent on the physical and chemical properties of the surface, such as surface free energy, surface charge, surface wettability, microstructure, rigidity, and hydrophobicity [2], duration of the incubation time, cell age, and temperature [3]. The effect of silicone in the body has been proven to be very stable in contact with physiological environments, and the LSR silicone implants compatible with tissues [7]. But, for long-term applications, there are huge differences can be found in the physical and mechanical behavior of silicone rubber, and when the application in the body is dynamic, the effect is even greater. Until now, two years was considered the maximum limit of use for an implantable silicone rubber device. This is due to the environmental stress cracking (ESC), the lack of light, or excessive heat, resulting in a very slow degradation of the implanted product. Several studies demonstrate that the body creates oxygen free radicals and monocytes, macrophages, fibroblasts, and collagenous tissue which encapsulate the device [5]. Figure 5 shows the encapsulation of a device after three months of implantation. When the macrophages are nearby, the concentration of H2O2 increases at the device surface, and for that reason, it is necessary to conduct additional experiments related to this scenario. Fortunately, H2O2 does not produce significant degradation in the silicone rubber. Additionally, the polymer is susceptible to auto-oxidation, changing the situation. When the polymer is in contact with metal in the device, and the latter decomposes or degrades, oxygen free radicals are generated due to the peroxide reaction with the metal. Another kind of degradation of the silicone rubber can occur during its application in the human body. Hydrolytic degradation is generated by enzymes, tissue pH, and/or physiologic ions. They change the silicone rubber structure, altering the dynamic properties of the silicone rubber. Mineralization occurs when the body deposits calcium salts on the device or creates an encapsulation.
Figure 5 Encapsulation of device formed by two layers: the first one has fibroblasts and collagen fibers, and the second one is made of inflammatory cells and blood vessels [11]
A clear way to determine the degradation of the silicone rubber are the changes in its mechanical properties. For example, the tensile stress decreases more than 10%, and the elongation at break increases the same value [12]. Also, swelling, yellowish color, loss of the shape, and environmental stress cracking are found. The absorbed species (biological fluids, blood lipids in the case of artificial heart valves) generate a plasticizing effect, and in consequence, a degradation of the material. Also, the crosslinking density changes and the sol content increases with the time of implantation, with the absorbed liquids being formed by low-molecular-weight polysiloxanes, and absorbed lipids, which confirms the cleavage of the backbone of the silicone rubber and the absorption of the corporal fluids in the silicone rubber [12]. This swells the material, although this absorption does not cause the failure itself because it does not exceed 1% wt. Some of these problems have been fixed by improving and optimizing the processing conditions focusing mainly on the curing and post-curing variables [12].
In some applications, comfort is an issue with the use of silicone rubbers. For instance, in maxillofacial prosthodontics applications, silicone rubber is not wetted by saliva, and it has frictional problems resulting in irritation, abrasion, and ulceration [17]. A simple solution would be the use of surfactants in the silicone rubber compound, however biocompatibility experiments must be conducted are necessary.
There are a handful of LSR molders that lead the field in injection molding Liquid Silicone Rubber. SIMTEC Silicone Parts, for example, is one of North America’s leading precision, high volume injection molders of medical grade and food grades and other grades of Liquid Silicone Rubber. SIMTEC is regarded as LSR experts that apply their knowledge, experience and advanced technology for the production of their customer’s LSR, two-shot, and multi-shot LSR products in life science (medical, healthcare, infant care), electronics, automotive and industrial markets.
References
- Rahimi, A., Mashak, A. Review on rubbers in medicine: natural, silicone and polyurethane rubbers. Plastics, Rubber and Composites, 42, 223-230, 2013.
- Fallahi, D., Mirzadeh, H., Khorasani, M.T. Physical, mechanical, and biocompatilibity evaluation of three different types of silicone rubber. Journal of Applied Polymer Science, 88, 2522-2529, 2003.
- Mirzadeh, H., Khorasini, M.T., Katbab, A.A., Burford, R.P., Soheili, Z., Golestani, A., Goliaei, B. Biocompatibility evaluation of laser-induced AAm and HEMA grafted EPR. Part 1: In vitro study. Clinical materials, 16, 177-187, 1994.
- Vert, M., Doi, Y., Hellwich, K.H., Hess, M., Hodge, P., Kubisa, P., Rinaudo, M., Schué, F. Terminology for bio related polymers and applications. Pure and Applied Chemistry, 84, 377-410, 2012.
- Stokes, K. Implantable neural prostheses 2 – Techniques and engineering approaches. Springer, 2010.
- Hassler, C., Boretius, T., Stieglitz, T. Polymers for neural implants. Journal of Polymer Science: Part B: Polymer Physics, 49, 18-33, 2011.
- Ikada, Y. Surface modification of polymers for medical applications. Biomaterials, 15, 725-736, 1994.
- Tiwari, A., Soucek, M.D. Concise Encyclopedia of high performance silicones. Scrivener Publishing LLC, 2014.
- Yoda, R. Elastomers for biomedical applications. Journal of biomaterials science, Polymer edition, 9, 561-626, 1998.
- Vondracek, P., Dolezel, B. Biostability of medical elastomers: A review. Biomaterials, 5, 209-214, 1984.
- Dolezel, B., Adamírová, L., Vondracek, P., Naprstek, Z. In vivo degradation of polymers. II. Change of mechanical properties and cross-link density in silicone rubber pacemaker lead insulations during long-term implantation in the human body. Biomaterial, 10, 387-392, 1985.
- Vince, V., Thil, M.-A., Veraart, C., Colin, I.M., Delbeke, J. Biocompatibility of platinum-metallized silicone rubber: in vivo and in vitro Journal of Biomaterials Science – Polymer Edition, 15, 173-188, 2004.
- Pedraza, E., Brady, A.-C., Fraker, C.A., Stabler, C.L. Synthesis of macroporous poly(dimethylsiloxane) scaffolds for tissue engineering applications. Journal of Biomaterials Science, Polymer Edition, 24, 1041-1056, 2013.
- Rey, T., Le Cam, J.-B., Chagnon, G., Favier, D., Rebouah, M., Razan, F., Robin, E., Didier, P., Heller, L., Faure, S., Janouchova, K. An original architectured NiTi silicone rubber structure for biomedical applications. Materials Science & Engineering C, 45, 184-190, 2014.
- Bai, H., Huang, C., Jun, L., Li, H. Modification of liquid silicone rubber by octavinyl-polyhedral oligosilsesquioxanes. Journal of Applied Polymer Science, 133, 43906, 2016.
- Stieghorst, J., Bondarenkova, A., Burblies, N., Behrens, P., Doll, T. 3D silicone rubber interfaces for individually tailored implants. Biomedical microdevices, 17, 54, 2015.
- Polyzois, G.L., Winter, R.W., Stafford, G.D. Boundary lubrication and maxillofacial prosthetic polydimethylsiloxanes. Biomaterials, 12, 79-82, 1991.